Dr. Catherine Hamlin: 90 Year Old Surgeon Keeps a Steady Hand in Ethiopia
Dr Hamlin says she will continue her work with women in Ethiopia with obstetric fistula.
Dr Hamlin says she will continue her work with women in Ethiopia with obstetric fistula.
VOA News By Joe DeCapua About 4,000 people are expected to attend this year’s International Conference on Family Planning. The…
New York’s PIX11 New York – Last week, Aster Degaro, a 13-year-old from Ethiopia had a life changing surgery to…
UNICEF Television September 13th, 2013 Gambella, Ethiopia – For a country that once made headlines for famine, poverty and war,…
Bogaletch Gebre’s work focuses on arranging “community conversations” on women’s issues in rural Ethiopia.
The DC Mayor’s Office on African Affairs invites you to an afternoon of health education workshops.
Clinic at a Time will hold a fundraiser this weekend at Lona Gallery in downtown Lawrenceville, Georgia.
Tadias Magazine Reader Submission By Yacob Gabremedhin Addis Ababa, Ethiopia – Imagine sitting quietly at a retreat center in Debre…
Ethiopia has transformed its system for tracking contraceptive sales from pins and pencils to computers and satellites.
The Word on Women – A second chance for Ethiopia’s child brides (Trust.org) By Jeff Edmeades Washington, DC – Once…
Ethiopia is benefiting from money brought home from abroad by Ethiopia’s returning diaspora.
World Bank is examining Nigeria, Ethiopia, Kenya and 19 other countries for a study on Universal Health Coverage.
The event was held last week at the United Nations in New York.
The first survey started this week in Oromia, in central Ethiopia where 22 million people live in suspected endemic areas.
2012 was a year when political leaders and top health officials freely spoke of attaining an AIDS-free generation.
Ethiopia moving to address doctor shortage but critics say corners being cut.
Last week I hosted the second public forum on mental health here in Washington, D.C.
Her most recent movie explores innovative ways to deliver healthcare to childbearing women in Ethiopia, Cambodia and Haiti.
A young Ethiopian doctor is starting the service in an attempt to improve access to health care.
I will be moderating a discussion on mental health in our community next weekend as we continue the conversation on the topic.
Science Blog Scientists say they have pinpointed genetic changes that allow some Ethiopians to live and work more than a…
The Guardian By Evelyn Owen Skilled and respected workers have revolutionised neighbourhood healthcare in Ethiopia – using a model other…
BCE (Battling Cancer in Ethiopia),is a U.K. based charity organization that aims to promote early cancer screening in Ethiopia.
Drink this regularly and everyone will think you’ve just returned from vacation in Awassa or Bahir Dar!
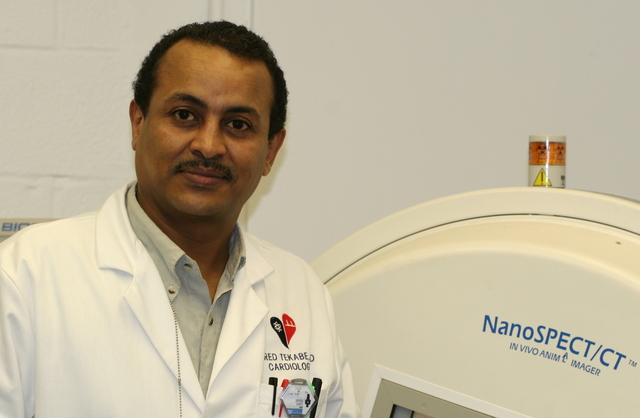
Dr. Tekabe’s research could potentially decrease the number of sudden deaths from heart attack.
As we welcome the Holiday season, we thought it worthwhile to take a moment to reflect on Ethiopia’s rich food traditions.
The Ethiopian American NGO Gemini Health Care Group’s upcoming mission to Ethiopia.
MSNBC correspondent Jenna Bush Hager shines light on maternal health in Ethiopia.
Above: Teff is gluten free and known for its flood and drought resistance. This year 150 acres was planted in…
Above: A quarter century after the 1984 famine, which left millions of Ethiopians destitute, familiar faces still linger as the…
The Huffington Post: My colleague Marc Cohen, a senior researcher at Oxfam America, reflects on the 25th anniversary since the…
Tekabe hopes that in a few years time his research can help heart disease prevention efforts and his laboratory has already received $1.6 million grant from the National Institute of Health.
Tadias Magazine By Dr. Asqual Getaneh & Dr. Adam Waksor Updated: Saturday, August 23, 2008 New York (TADIAS) – Every…
Although the expansion of modern medicine appears to influence some aspects of the traditional system, traditional Ethiopian medicine remains rooted in magico-religious beliefs and empirical knowledge from the natural environment.